Patients in need of gall bladder removal often choose a laparoscopic (less invasive) approach for their cholecystectomy. This is because, in general, laparoscopic patients benefit from reduced pain, faster return to normal activities, and reduced risk of surgical site infection with a laparoscopic approach compared to an open operation.
Unfortunately, despite the upsides, bile duct injury rates after gall bladder removal surgery have increased since the introduction of laparoscopic cholecystectomy, occurring in about 3 per 1,000 procedures performed. As many Pittsburgh, Pennsylvania patients have learned, bile duct injuries after cholecystectomy can be life altering with complications leading to additional surgeries, pain and discomfort, shortened life expectancy and death.
One of the most devastating injuries sustained by patients undergoing laparoscopic cholecystectomy surgery is injury to the common bile duct. As medical malpractice lawyer Jerry Meyers has written about in the past, patients with cut bile duct injuries after surgery should assume their injury was the result of medical malpractice until proven otherwise.
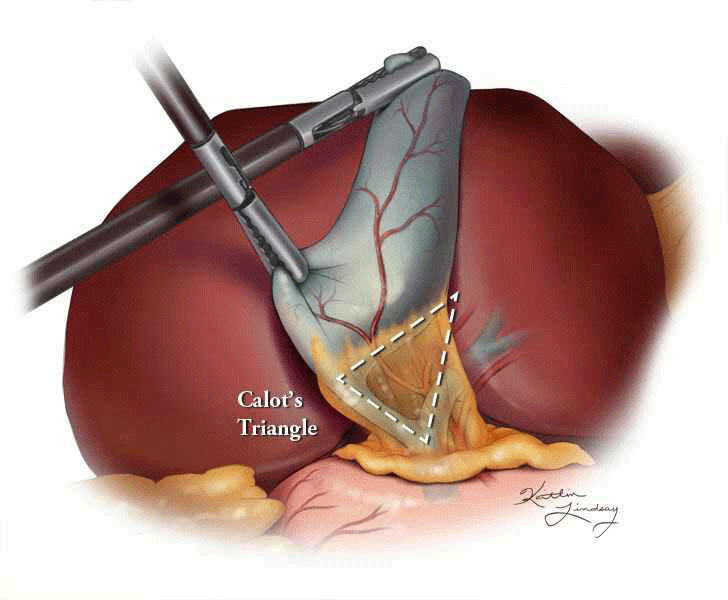
Almost universally, the most common cause of injury to the common bile duct is the doctor’s failure to identify the structures of the Triangle of Calot. More than 2/3 of injuries are due to an inadequate Calot’s dissection leading to confusion of normal anatomy.
In order to end this avoidable complication, the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has developed a strategy for minimizing devastating bile duct injuries. The SAGES Safe Cholecystectomy Program recommends the following strategies for minimizing bile duct injuries (for more details, please refer to their website):
- Use the Critical View of Safety (CVS) method of identification of the cystic duct and cystic artery during laparoscopic cholecystectomy.
- The hepatocystic triangle is cleared of fat and fibrous tissue.
- The lower one-third of the gallbladder is separated from the liver to expose the cystic plate.
- Two and only two structures should be seen entering the gallbladder. Use a Doublet view (anterior and posterior images)
- Perform an intra-operative time-out during laparoscopic cholecystectomy prior to clipping, cutting or transecting and ductal structures.
- Understand the potential for aberrant anatomy in all cases.
- Make liberal use of cholangiography or other methods to image the biliary tree intraoperatively.
- Recognize when dissection is approaching a zone of great danger and halt the dissection before entering the zone. Finish the operation by a safe method other than cholecystectomy if conditions around the gallbladder are too dangerous.
- Get help from another surgeon when the dissection or conditions are difficulty.
These are simple straightforward steps that your surgeon should follow in order to avoid a life changing injury to you or your loved one’s bile duct. If you or a loved one has been diagnosed with a cut, severed or injured bile duct after undergoing a laparoscopic cholecystectomy it is important to investigate the surgeon’s operative record to see if all the required safety steps recommended by SAGES were followed. If not, the this devastating injury was likely avoidable and there may be a strong basis for a medical malpractice settlement or lawsuit.
*Jerry Meyers retired from the firm in 2021.