Delayed Diagnosis of Bowel Perforation
Bowel perforation is a serious medical condition where a hole forms in the wall of the intestines. A perforated bowel can lead to a bowel leak which spills intestinal contents like fecal matter inside the abdomen or pelvis. A bowel leak can lead to life-threatening complications if not promptly diagnosed and treated. If an opportunity for treatment was lost due to a delay in diagnosis, a lawsuit may be warranted.
In many instances, bowel perforation or leak is a result of medical conditions affecting the small or large intestines, abdominal or pelvic surgery, or diagnostic procedures like colonoscopy. The lawyers of Lupetin and Unatin, LLC have helped several victims of bowel injury or their families understand their rights and navigate the complexities of their cases. This article outlines common situations leading to bowel perforation or bowel leak and ways in which the diagnosis and treatment may be delayed.
Case Study: Justice After A Preventable Bowel Perforation
In the realm of medical malpractice, few cases illustrate the fragility of health and the catastrophic impact of a single decision like the case of “Eleanor.” An 80-year-old widow residing in Erie, Pennsylvania, Eleanor was the picture of vitality and independence—until a trip to the emergency room for severe constipation turned into a life-threatening nightmare. Due to a failure to properly interpret imaging studies and the negligent prescription of a dangerous laxative, Eleanor suffered a perforated colon, septic shock, and months of agony and embarrassment.
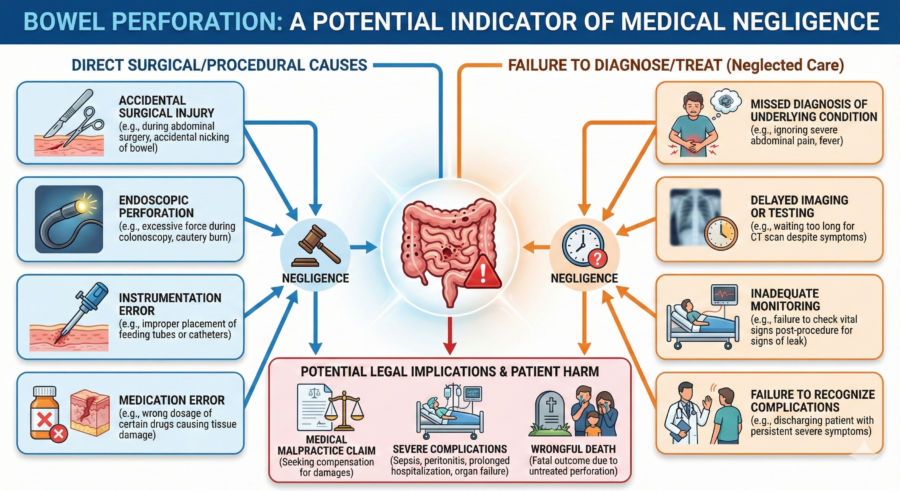
Common Causes of Bowel Perforation
Bowel perforation or leak can occur due to a variety of medical and surgical situations. It is important for doctors and nurses to know when a patient has an increased risk of bowel perforation due to one or more of the following medical conditions or surgical procedures.
Surgical Errors and Complications
Surgical procedures involving the abdomen, such as appendectomies, colonoscopies, and laparoscopic hernia repair, carry a risk of accidentally perforating the bowel. Bowel injury can also occur during pelvic surgery involving gynecologic surgeries such as total hysterectomy. Factors which increase the risk of bowel injury include extensive scar tissue from prior surgery and higher complexity of the surgery.
Lack of proper technique, inadequate training, or failure to recognize and repair the perforation during surgery can be grounds for a malpractice claim. But not all bowel injuries are immediately apparent during surgery. During surgery the outer surface of the bowel wall may be nicked, but not perforated through the entire thickness of the bowel wall at the time of surgery. This superficial injury can be missed by the surgeon when they inspect the bowel for injury at the conclusion of the surgery.
Then, in the hours and days after surgery, the injury to the bowel may worsen until it forms a full-thickness perforation through the bowel wall, leading to a bowel leak. Surgeons must keep a high-level of vigilance for signs and symptoms of bowel perforation or bowel leak in the hours and days after surgery in the event full perforation of the bowel wall develops in the post-operative setting.
Delayed Diagnosis of Gastrointestinal Conditions
Conditions like diverticulitis, Crohn’s Disease, prolonged small bowel obstruction, hernias, volvulus, and peptic ulcers can lead to bowel perforation if not diagnosed and treated in a timely manner. Misdiagnosis, delayed diagnosis, or failure to follow up on critical symptoms may constitute medical negligence.
Endoscopic procedures and interventions
Endoscopic procedures, which involve inserting instruments into the gastrointestinal tract, can cause perforation. Bowel perforations can occur due to improper handling of instruments, or the failure to properly handle situations which arise during this procedure and increase the risk of injury to the bowel. Most often, endoscopic procedures are performed in a safe manner. Still, therapeutic treatments during the procedure such as removal of polyps or treatment of ulcers in the intestinal tract can expose the patient to an increased risk of a delayed intestinal perforation or bowel leak.
Infections and Inflammatory Conditions
Severe infections like appendicitis or inflammatory conditions can weaken the bowel wall, leading to perforation and leakage of intestinal contents. Failure to diagnose and treat infections or inflammatory conditions promptly can result in perforation and potential malpractice claims.
Recognizing Signs and Symptoms of Bowel Perforation
Early recognition of the signs and symptoms of bowel perforation or bowel leak is crucial for prompt medical intervention. Symptoms often include severe abdominal or back pain, fever, nausea, vomiting. Abnormal lab results on a complete blood count or elevated C-reactive protein can be signs of an infectious or inflammatory reaction from a perforated bowel. Imaging studies like abdominal x-rays or, more often CT scans, may show evidence of free gas, fluid, or an abscess in the abdomen. If the cause of these signs and symptoms is not promptly investigated, the condition can rapidly worsen, leading to severe complications or death.
Delays in the diagnosis of bowel perforation or leak can occur due to various other factors. The most common reasons for these delays include:
Inadequate Patient Histoy and Physical Examination
A thorough patient history and physical examination are essential for diagnosing bowel perforation and a resultant leak. In some cases, busy clinical settings or incomplete patient information can result in a less comprehensive evaluation.
Sudden and severe abdominal or back pain is often the first sign of a bowel perforation and leak. Severe abdominal or back pain occurring after a procedure involving the GI tract should lead doctors to suspect an injury to the GI tract. Too often, nurses and doctors assume when a patient complains of pain after surgery, it’s just related to the incisions related or the underlying problem the surgery was intended to address rather than a perforated bowel.
Invasive surgery certainly causes pain, especially in major abdominal operations like gastric bypass or removal and reattachment of bowel. But sometimes, doctors and nurses assume any and all pain after surgery is normal, and they don’t take the time to learn when the patient’s pain is out of proportion to the surgery itself. Doctors and nurses should ask important questions like these to make sure a perforated bowel with bowel leak is not the source of the patient’s pain:
- Is the patient’s abdominal pain similar or different from prior bouts?
- Is the patient’s post-op pain significantly worse compared to the patient’s pain in the first day or two after surgery.
- Is the pain in the same location as the incision or a slightly different location of the body?
Bottom line: it’s never safe to assume sudden, severe abdominal or back pain is normal if it starts suddenly in the hours or a days after surgery on the gastrointestinal tract.
Protect Yourself! It is extremely important for the patient, if able, or a family member to tell doctors and nurses if they are concerned about their pain. The patient or their loved ones are often the best advocates for the patient and should raise their voices when pain or other symptoms are new, seem unusually severe, or possibly related to an unexpected complication.
Failure to Recognize the Signs of Bowel Perforation and Leak on Radiology Studies
Often, the diagnosis of potential bowel perforation is made through the performance of an abdominal x-ray or CT scan. Worrisome findings include unexpected levels of free air or fluid in the abdomen near the site where the surgery was performed. In some cases, an infectious mass known as an abscess can form within the abdomen at the site of a perforation where a bowel leak has occurred.
At Lupetin and Unatin, we have seen multiple cases where doctors either delayed ordering abdominal imaging despite symptoms of bowel leak or underappreciated findings like free air or fluid in the abdomen. In the proper setting, abnormal radiology findings are a red flag to take a patient back to the operating room for exploratory surgery to look for a bowel perforation. If a surgeon fails to follow-up on the results of diagnostic testing like radiology studies or delays exploratory surgery despite reason to suspect a bowel perforation and leak, and the patient suffers great harm, the surgeon and the hospital may be responsible for the consequences.
Communication Breakdown Among Healthcare Providers
Effective communication among healthcare providers is crucial for timely diagnosis and treatment. Breakdowns in communication can occur between nursing staff and physician, or between different departments, such as the radiology department and the unit where the patient is receiving treatment. Miscommunication or lack of information sharing can lead to delays in recognizing and treating bowel perforation and leak.
Cognitive Biases
Cognitive biases, such as anchoring (focusing on pain from the surgery itself or the underlying condition leading to surgery, or dismissing free air in the abdomen as related to insufflation of the abdomen during laparoscopic surgery) and availability bias (relying on readily available information, like focusing on a normal abdominal x-ray, even though x-rays often do not show the early signs of bowel perforation as well as a CT scan), can influence a healthcare provider’s diagnostic process. These biases can lead to misdiagnosis and delays in considering bowel perforation or bowel leak as a potential cause of symptoms.
Legal Grounds for Medical Malpractice Claims
Proving medical malpractice in cases of bowel perforation with leak involves establishing that the healthcare provider deviated from the standard of care, directly causing the injury. Key elements include:
- Duty of Care: Establishing that the healthcare provider owed a duty of care to the patient.
- Breach of Duty: Demonstrating that the provider breached this duty by failing to meet the standard of care.
- Causation: Proving that the breach directly caused the bowel perforation and resulting harm.
- Damages: Documenting the physical, emotional, and financial damages suffered by the patient.
The lawyers of Lupetin and Unatin have successfully represented clients in lawsuits involving the death of patients whose doctors delayed the diagnosis of a bowel perforation. Cases our firm has handled include:
- $3 million-dollar settlement on behalf of the widow of a man who developed abdominal infection and died after surgery to remove a diseased portion of his colon;
- $400,000 settlement on behalf of the estate of a woman who developed symptoms of a bowel injury after hernia repair surgery. The signs of peritonitis and sepsis were overlooked by her doctors and nurses, leading to her unfortunate death and great loss to her siblings.
Conclusion
Delays in diagnosis of bowel perforation or a bowel leak can result from a combination of patient-related, provider-related, and systemic factors. Addressing these issues involves improving clinical protocols, ensuring thorough patient evaluations, enhancing diagnostic accuracy, and fostering effective communication among healthcare providers. Understanding these common causes can help in taking proactive steps to minimize delays and improve patient outcomes.
If you or a loved one has suffered due to a delayed diagnosis of bowel perforation or bowel leak, it is essential to seek legal advice to understand your rights and potential avenues for compensation If you would like to discuss the specifics of your case, please reach out to us at Lupetin & Unatin, LLC.